





What is an inpatient comprehensive assessment for the purposes of the National Audit of Inpatient Falls (NAIF)?
NICE clinical guideline 249 recommend comprehensive assessment for:
- All hospital inpatients aged 65 and over
- Hospital inpatients aged 50-64 with a condition that increases the risk of falling.
NAIF includes all inpatients aged 65 and over who have sustained any fracture or a head or spinal injury as a result on an inpatient fall and collects information about six components of the comprehensive assessment (which contribute to the Multi-factorial Assessment to Optimise Safe Activity – MASA). The reason for this is to minimise data collection burden and to reflect assessments and actions thought to have the strongest effect on fall prevention.
Although we are only collecting data on six actions, we strongly recommend that all hospitals to offer a comprehensive falls assessment to identify the patients' individual fall risk factors:
- Vision
- Cardiovascular
- Delirium
- Medication review
- Gait, balance and mobility, and muscle strength assessment
- Urinary continence
- Alcohol misuse
- Cognition
- Mood
- Diet, fluid intake and weight loss
- Dizziness
- Footwear and foot condition
- Functional ability
- Hearing impairments
- Neurological examination
- Osteoporosis risk assessment.
Clinicians can access a guide for comprehensive assessment for inpatients.
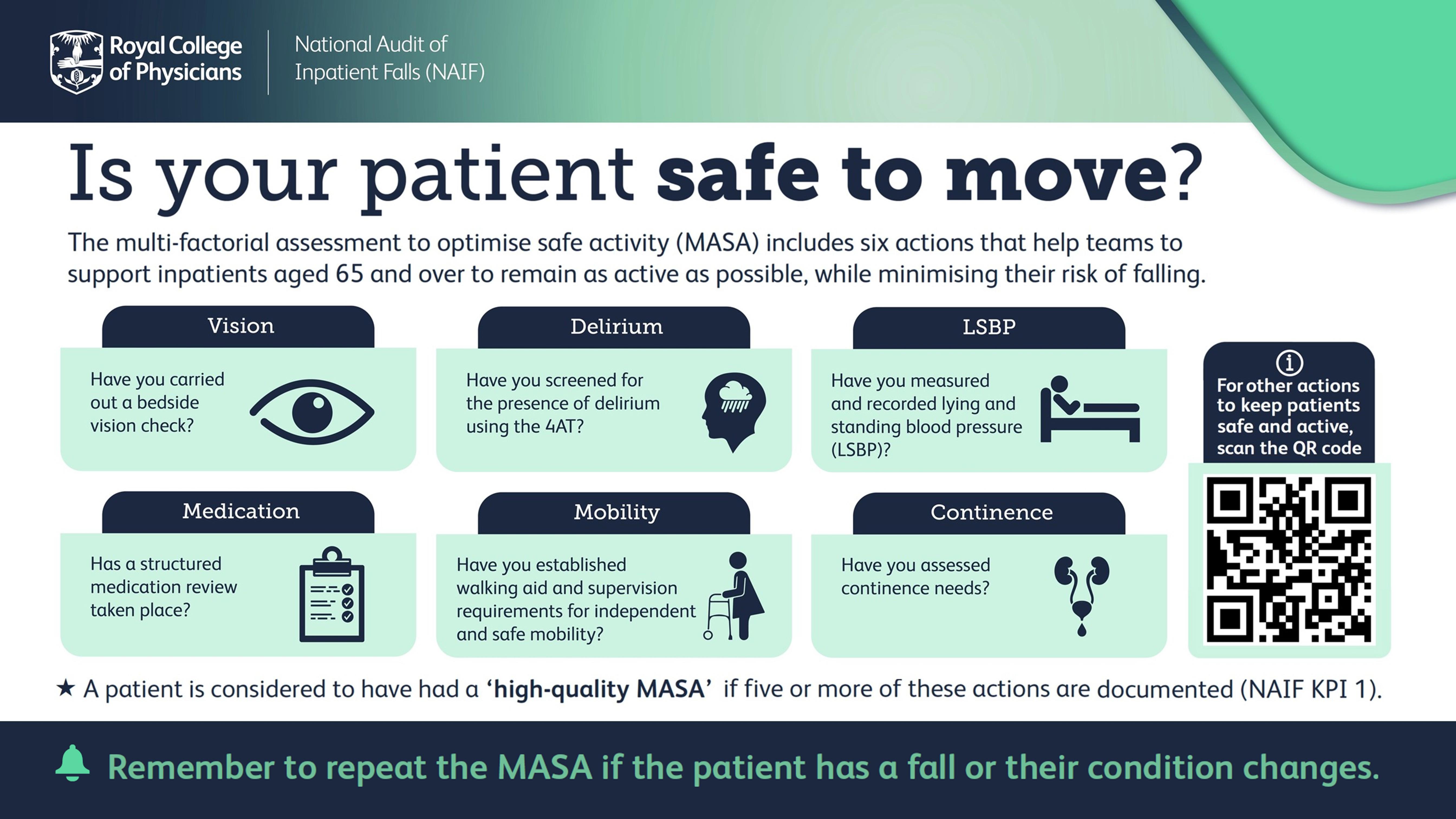
Multi-factorial assessment to optimise safe activity (MASA)
The purpose of the Multifactorial Assessment to optimise Safe Activity (MASA) is to prepare and encourage a hospitalised older adult to be as active as possible by identifying and addressing issues that may compromise their safety when moving around. We hope that positive communication concerning being active, rather than the more negative message of preventing a feared event (a fall), will enable staff, patients and families to feel confident in preventing hospital-acquired deconditioning, while minimising falls.
The first six components of the MASA are considered to be a minimum standard for an assessment to be described as a MASA within the scope of NAIF. A patient who has five or more of these factors assessed will be considered to have had a ‘high quality MASA’. This is the first Key Performance Indicator for NAIF.
The NAIF team recognise that physical activity levels are very low in people admitted to hospital. Research suggests that inpatients spend 87–100% of the day in bed or sitting and on average, older inpatients take around 600 steps a day. This is a fraction of that recommended for good health and research has found that step count doubles the day after older people are discharged home.
The physical inactivity imposed by hospitalisation is associated with rapid deconditioning leading to functional decline, more readmissions and increased mortality. These effects are particularly pronounced in older people – the group of patients most likely to experience an inpatient fall.
Around 30% of older inpatients will experience hospital-acquired deconditioning (HAD) and it should be considered as a significant potential harm for older people in hospital.
The way in which hospital staff consider falls risk in the context of physical activity is a key driver of HAD. Due to the nature of the human movement (where there is a small base of support and high centre of gravity), standing up and walking notably increases the possibility a fall will occur. Therefore, an understandable instinct is to seek to reduce falls by limiting time spent upright and moving. However, this approach is flawed as the muscle weakness, loss of balance skill and reduction in general fitness caused by HAD will not only further increase the risk of falls, it will expose patients to similar if not greater levels of harm from the range of negative consequences.
MASA poster - Is your patient safe to move?
- PDF with print crop
- PowerPoint slide (no animation)
- PowerPoint slide (with animation)
- Screensaver (JPG)
{kind=link}
Resources to support MASA:
Six components of the MASA:

 Assessment process / question / tool
Assessment process / question / tool
- Ask about spectacle use
- Measurement of distance and near visual acuity using the ‘Look Out’ vision tool.
Intervention to address component
During inpatient admission:
- Ensure access to own, clean spectacles
- Appropriate supervision in new environment for people with severe visual impairment.
- Keep ward areas and toilets well lit, clear of clutter, trip or slip hazards.
- Provide colour coding to bays / rooms and clear signage for toilets and other facilities.
- Use adequate contrast between colours of equipment, décor, walking aids for people with visual impairment (local adaptations advised depending on resource availability).
- Provide information and educational materials for the patient and their family. NAIF patient resources are available here.
For discharge:
- Advise about eye tests and spectacles
- Referral for cataract extraction if indicated.
 Assessment process / question / tool
Assessment process / question / tool
- Perform and record LSBP measured as per the RCP guide (including measurement of pulse).
Intervention to address component
During inpatient admission, if orthostatic hypotension identified:
- Review medication
- Assess fluid balance / hydration
- Manage medical causes such as sepsis
- Formalise strategies to minimise impact (i.e. sitting up slowly)
- Consider compression socks and stockings.
Further investigations as appropriate if there is evidence of syncope.
 Assessment process / question / tool
Assessment process / question / tool
- Screen using 4 assessment test (4AT)
For more recommendations around diagnosing and treating delirium, read NICE guideline for delirium (CG103).
Intervention to address component
During inpatient admission: Manage underlying cause of delirium including:
- Awareness of how to identify unmet needs they may not be able to easily express, use the “This is me” document.
- Alternative methods to using the call bell / remembering verbal instructions if supervision or assistance is needed to walk.
- Provide person-centred occupation appropriate to abilities to alleviate boredom.
- Continence management plan may include a toileting routine, intentional rounding, management of constipation, hydration and medication.
- Provide information and educational materials for the patient and their family – available here.
For discharge:
- Consider community follow up of for patients with unresolved delirium on discharge.
 Assessment process / question / tool
Assessment process / question / tool
Structured medication review that identifies medications that could potentially increase falls risk and assesses the clinical indication for deprescribing or withdrawal.
Such a review may, in some cases, recommend starting a new prescription.
Validated tools are available to carry out a structured medication review.
Intervention to address component
During inpatient admission:
- Document actions where changes to prescriptions are made to reduce risk drugs, new prescriptions started or provides a rationale to continue a drug associated with risk of falls is provided.
- Provide information and educational materials for the patient and their family – available here.
For discharge:
- Ensure medications changes are clearly communicated to the primary care team (and care home, if appropriate).
 Assessment process / question / tool
Assessment process / question / tool
Walking and transfer assessment which includes:
- Supervision / assistance requirements for transfers and walking
- Equipment and walking aids required for transfers and walking
- Risks contributing to deconditioning.
Intervention to address component
During inpatient admission:
- Care plan to specify how supervision and assistance will be provided to ensure the patient can remain as active as possible.
- Mobility aids (if needed) to be in reach of the patient.
- Ensure bed and chair heights are optimised for each patient and that if used, bed rail assessments are completed.
- Appropriate equipment for moving and handling to be available on the ward and in working order.
- A personalised care plan in place to optimise physical activity and reduce sedentary time during the admission.
- Ensure appropriate clothing and footwear for moving around is available.
- Provide information and educational materials for the patient and their family – available here.
For discharge:
- Consider referral for community fall prevention exercise.
 Assessment process / question / tool
Assessment process / question / tool
- Question about / observation of continence, any accidents, urgency, frequency and use of pads.
- Note any change in continence associated with the hospital admission.
Intervention to address component
During inpatient admission, continence care plan which may include:
- Supporting adequate hydration
- Supporting with toileting, using the toilets on the ward as the default approach
- Avoidance of urinary catheters with clear justified reason for their use
- Review of the anticholinergic effect of medications used to manage bladder conditions and consideration of alternatives
- Considering non-pharmacological approaches such as pelvic floor muscle training and bladder training to manage urinary incontinence.
!! Do not use pads to compensate for reduced mobility.
For discharge:
- Ensure appropriate community management, including continuation of pelvic floor / bladder training and/or community pad provision and equipment needs (i.e. bottle / commode).
NAIF recommends repeating the MASA weekly, or sooner if the patient has a recent fall or any change in condition.
Other comprehensive assessment components
as per NICE clinical guidelines 249
For more recommendations around diagnosis, assessment and management of harmful drinking (high-risk drinking) and alcohol dependence, read relevant NICE guideline CG115.
Assessment process / question / tool
- Record history of alcohol intake to identify those with history of harmful or hazardous drinking.
- Assess for symptoms of / determine the risk of acute alcohol withdrawal while admitted.
Interventions to address component
During inpatient admission:
For discharge:
- Education / support for withdrawal.
Assessment process / question / tool
Note any history of cognitive impairment / dementia in health records or reported by the patient or their family.
Interventions to address component
During inpatient admission: see interventions for delirium (relevant NICE guideline).
For discharge: Consider community follow up of for patients with new cognitive impairment while in hospital.
Assessment process / question / tool
- Note BMI and any recent weight loss to calculate Malnutrition Universal Screening Tool (MUST) score.
- Identify and record any reasons why oral intake of food and fluids may be impaired.
Interventions to address component
During inpatient admission:
- Care plan to support adequate nutrition and fluid intake.
- Investigate reasons for weight loss and implement interventions to address malnutrition if indicated.
Read relevant NICE guideline NG127.
Assessment process / question / tool
Ask about the presence and nature of any dizziness.
Interventions to address component
During inpatient admission, investigation of causes including:
- Lying / standing blood pressure
- Cardiovascular examination
If suspected vertigo and appropriate for the patient’s condition, consider a Dix-Hallpike manoeuvre.
For discharge :
- Consider referral for further investigation and/or treatment of vertigo.
Assessment process / question / tool
- Ascertain whether footwear is missing or unsuitable.
- Visual inspection of the feet for foot problems that impact on walking.
Interventions to address component
During inpatient admission:
- Arrange for patients to have access to their own suitable clothing and footwear during the admission.
- Support the necessary footcare for maintaining mobility while an inpatient.
For discharge:
- Consider referral to community podiatry or footcare services.
Assessment process / question / tool
- Assess the person's perceived functional ability and explore any concerns about falling.
- Ask if the patient is concerned about falling.
Interventions to address component
During inpatient admission:
- Consider short-form FES-I to establish how concern about falling impacts on perceived ability to undertake functional activities.
- Consider any concerns about falling that may lead to activity limitation, while in hospital, in the mobility care plan.
For discharge:
- Consider referral for community fall prevention exercise.
Assessment process / question / tool
Question about any hearing difficulties and hearing aid use.
Interventions to address component
During inpatient admission:
- Ensure hearing aids (if used) are available and in working order. Use adaptations to support communication as indicated.
- Examination for earwax.
For discharge:
- Consider referral for hearing aids or further audiology assessment if indicated.
Assessment process / question / tool
Note any history of mood disorders / depression in health records or reported by the patient or their family.
Intervention to address component
During inpatient admission:
- Further investigation using Geriatric Depression Scale-15
- Consider specialist assessment / management if mood disorder is impacting on mobility and rehabilitation or prescribed antidepressants are thought to be contributing to fall risk.
Assessment process / question / tool
- Can the patient move all four limbs normally?
- Any abnormalities in walking or balance that cannot be explained by current condition?
Interventions to address component
During inpatient admission:
- If impairments in movement noted arrange for healthcare professional (with appropriate skills) to perform neurological assessment including tone, reflexes, sensation, motor function, cranial nerves.
- Investigate unexplained signs and symptoms as appropriate.
Read relevant NICE guideline CG146 which covers assessing the risk of fragility fracture in people aged 18 and over with osteoporosis.
Assessment process / question / tool
- Was the patient is admitted with a fracture (or sustained a fracture while in hospital)?
Interventions to address component
During inpatient admission:
- Perform FRAX and follow osteoporosis NICE guidance. If clinically indicated, start on bone therapy while still in hospital.
- If indicated, consider dose of IV bisphosphonate before discharge where adherence to oral bisphosphonates in the community is likely to be challenging.
For discharge:
- Referral for further investigation / management if indicated at discharge.